
Clinical background
Etiology: Human dirofilariasis is caused by Dirofilaria repens (subcutaneous/ocular) and Dirofilaria immitis (pulmonary). Humans are accidental, dead-end hosts.
Transmission: Mosquito-borne from infected dogs or wild carnivores.
Presentation: 1. D. repens: Subcutaneous or ocular nodules, often painless.
2. D. immitis: Pulmonary “coin lesions,” usually asymptomatic.
Lab findings: Peripheral eosinophilia is inconsistent. Serology is unreliable. Imaging may show well-defined nodules but is often nonspecific. Ultrasound—well‑defined hypoechoic lesion with a linear, mobile echogenic structure (“filarial dance” may be absent in Dirofilaria)
Presenting complaints: Painless or mildly tender subcutaneous/ocular nodule; occasionally pruritus or local swelling. If pulmonary, incidental “coin lesion” on imaging.
Gross pathology
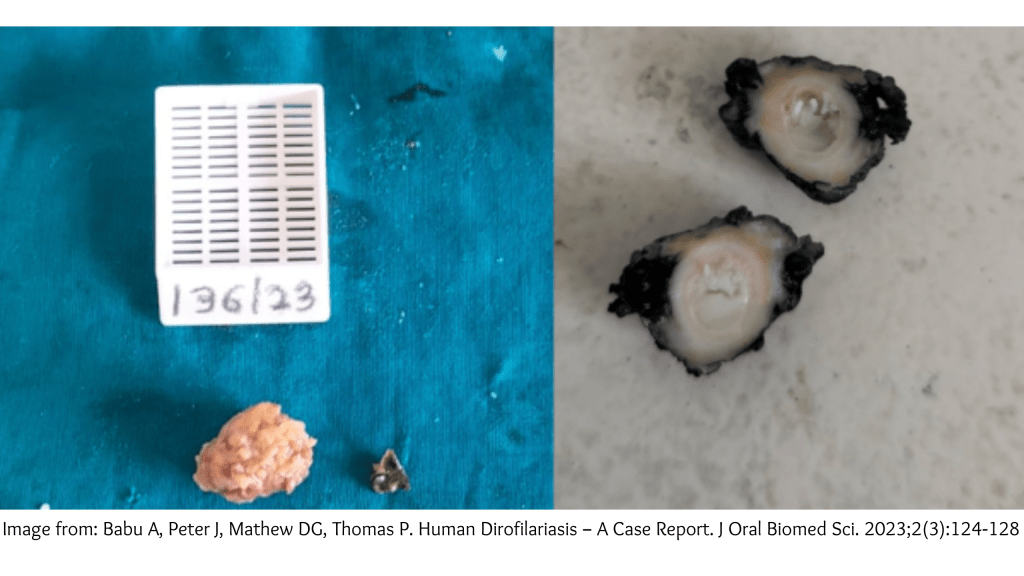
Specimen: Excision biopsy of subcutaneous/ocular nodule (rarely pulmonary wedge resection).
Macroscopy: Firm, well‑circumscribed nodule, 0.5–2.0 cm; cut surface shows fibrous tissue with a slender, whitish, thread‑like structure (worm) within a cystic or fibrotic cavity; minimal necrosis.
Microscopy:
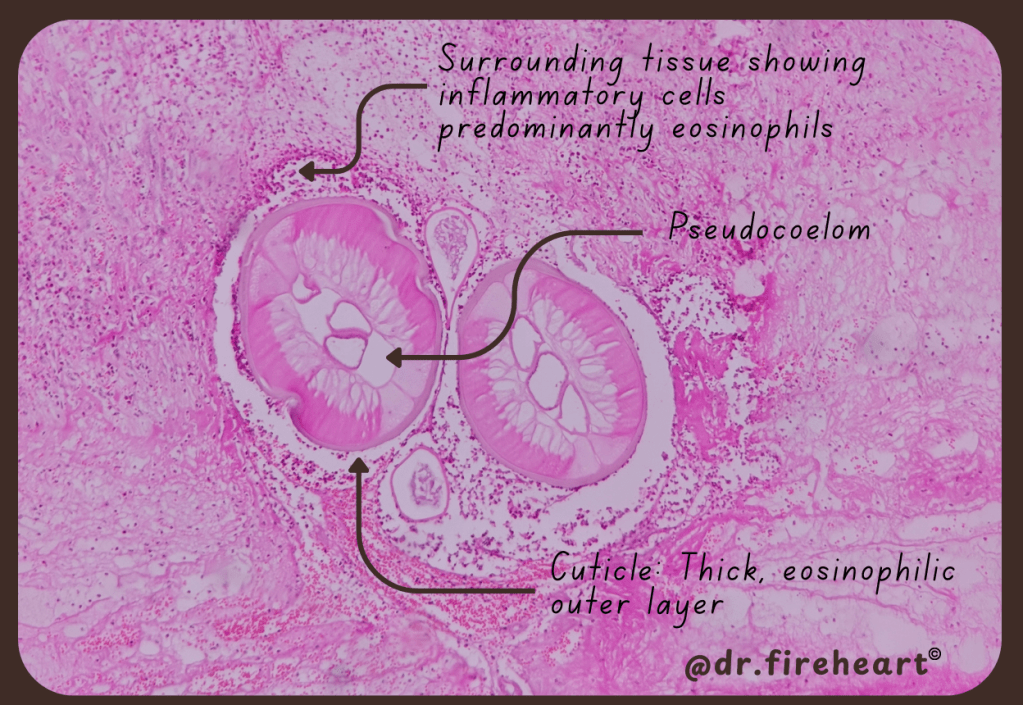
Architecture & cellular details: Transverse sections of a nematode with:
1. Thick, eosinophilic multilayered cuticle with subtle longitudinal ridging.
2. Prominent lateral chords, peripheral somatic muscle layer.
3. Internal organs—paired uteri (often with ova/microfilariae), intestine, and pseudocoelom.
4. Host response—mixed inflammatory infiltrate with eosinophils, lymphocytes, plasma cells; early fibrotic encapsulation; granulomatous reaction may be present.
Special features: No significant atypia; mitoses not relevant. Necrosis may be focal due to degeneration of the worm.
Differential diagnoses (morphology):
1. Other filarial nematodes (e.g., Wuchereria, Brugia, Onchocerca)—differ by cuticular ridging pattern, size, tissue predilection.
2. Sparganosis (plerocercoid tapeworm)—lack of thick ridged cuticle; parenchymal body with calcareous corpuscles.
3. Cysticercosis—scolex/tegument; calcareous corpuscles; cyst wall.
4. Loa loa—subcutaneous migration; different cuticular features.
Ancillary Studies
Special stains: Routine H&E is usually sufficient. PAS may accentuate cuticle; Giemsa can highlight microfilariae.
Molecular: PCR on tissue for species‑level identification (e.g., D. repens vs D. immitis); sequencing of mitochondrial/ITS regions if available.
Discussion:
Pathogenesis: Zoonotic infection—humans are accidental, dead‑end hosts. Mosquito vectors transmit Dirofilaria from canine reservoirs; larvae fail to complete their life cycle in humans, localizing as solitary nodules.
Diagnostic dilemmas: Fragmented/degenerate worms can obscure key features; distinguishing Dirofilaria from other helminths relies on cuticular ridging, lateral chords, and reproductive structures. Molecular confirmation is helpful when morphology is limited.
Management and outcome:
Treatment: Complete surgical excision of the nodule.
Follow‑up: Excellent prognosis; recurrence is uncommon. Evaluate for additional lesions only if symptoms suggest.
Take‑home messages:
Diagnostic pearl: Thick multilayered cuticle with subtle longitudinal ridges, lateral chords, somatic muscle, and paired uteri point to Dirofilaria.
Pitfall: Degenerate fragments can mimic other helminths—use overall anatomy, not single features; consider PCR if morphology is equivocal.
Broader relevance: Human dirofilariasis is not rare in endemic regions—recognizing it avoids unnecessary oncologic workups and reassures patients with a curable, benign outcome.
Sources:
- Annoor Journal of Oral & Biomedical Sciences. Human dirofilariasis: a case report. Annoor Journal of Oral & Biomedical Sciences; [cited 2026 Jan 19]. Available from:
https://annoorjournal.org/journals/human-dirofilariasis-a-case-report/ - Journal of Clinical and Diagnostic Research (JCDR). Ocular dirofilariasis case from Mumbai. JCDR; [cited 2026 Jan 19].
- Europe PMC. Ocular dirofilariasis clinicopathologic series. Europe PMC; [cited 2026 Jan 19]. Available from:
https://europepmc.org/article/MED/38751499

Leave a comment